Colon
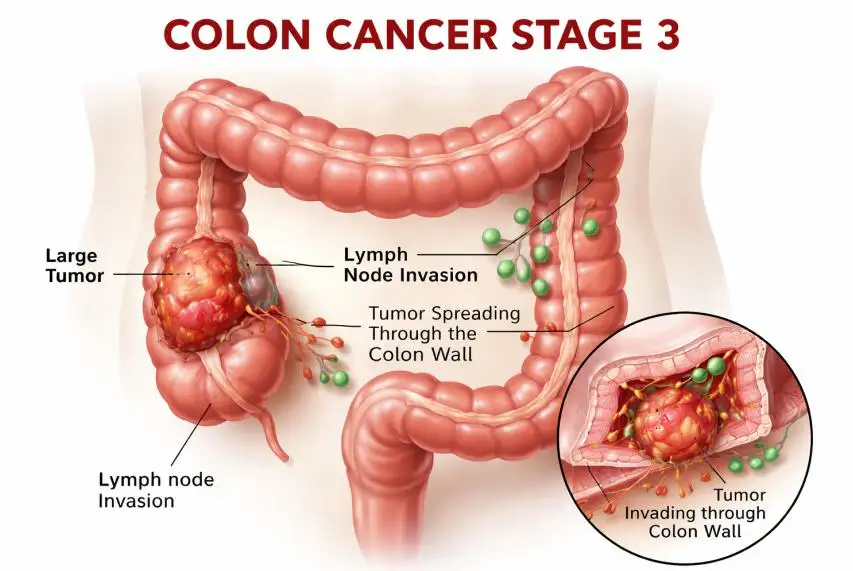
Stage 3 Colon Cancer Treatment: Complete Guide to Options, Survival, and Recovery
Stage 3 colon cancer treatment plays a critical role in improving survival and preventing the spread of cancer to other…